Services
Physiotherapy

Once the diagnosis is made, a treatment plan is then discussed and implemented. Treatment frequently involves a combination of manual (hands on) therapy, together with a tailored rehabilitation programme. Other modalities such as ice/heat, taping/strapping/bracing, and electrotherapy are all used as necessary to reduce inflammation and encourage the body’s natural healing process.
Achievement of short and longer term goals are always the focus and these will be regularly discussed with you throughout the management of your injury.
Post Operation Rehabilitation

Throughout my career so far, I have gained vast experience in rehabilitating patients after a wide range of orthopaedic procedures. In that time, I have developed close working relationships with many of the area’s best orthopaedic surgeons, and regularly receive referrals from them whether it is for rehabilitation following a procedure, or for conservative management of an injury with a view to avoiding surgery. Often patients will be referred for physiotherapy prior to an elective procedure for what has become known as ‘prehab’ and this not only allows them to go into an operation in the best possible condition allowing for quicker recovery afterwards, but it helps to familiarise them with what is going to happen in the immediate post op period. This has proved to be incredibly useful and whenever it is possible to do it, it is highly recommended. The following list includes the most common orthopaedic procedures that I see, but the list is not exhaustive. If you have an upcoming operation and you would like to discuss the physiotherapy aspect of it, please get in contact.
Foot and ankle
Bunion surgery, cheilectomy, ankle arthroscopy, lateral ligament repair/stabilisation, tendon repair (with or without graft), internal fracture fixation, joint fusion (ankle joint, subtalar joint, big toe).Knee
Total or unicompartmental knee replacement, arthroscopic meniscus repair/meniscectomy, ACL reconstruction, MCL repair, multiple ligament reconstruction, patellofemoral joint stabilisation (medial patellofemoral ligament repair), high tibial osteotomy, microfracture/debridement of chondral lesions.Hip
Total hip replacement/resurfacing, labral repair, arthroscopic debridement of femoral cam lesions.
Spine
Facet joint and epidural injections, lumbar or cervical decompression, fusions.Shoulder
Subacromial decompression, rotator cuff repair, anterior stabilisation (Bankart lesions), SLAP repair, biceps tendon repair/tenotomy, acromioclavicular joint (ACJ) excision, ACJ stabilisation, most manipulation/arthroscopic capsular debridement for frozen shoulder.Elbow
Arthroscopic debridement, tennis/golfers elbow release, cubital tunnel release.Hand/wrist
Trigger finger release, Dupuytrens contracture, carpal tunnel release, trapeziectomy.Trauma
Routine or complex fracture fixation (internal, or external fixators such as Ilizarov frames, conservatively (non operatively) managed fractures, tendon repairs after acute rupture.Post steroid injections
Many musculoskeletal injuries are suitable for treatment with a steroid injection. This is usually the case where conservative treatment has, or is likely to fail, but surgical intervention is not yet warranted. Almost all of these warrant physiotherapy follow up to make the most of any benefits in pain reduction achieved by the injection.Ultrasound Imaging
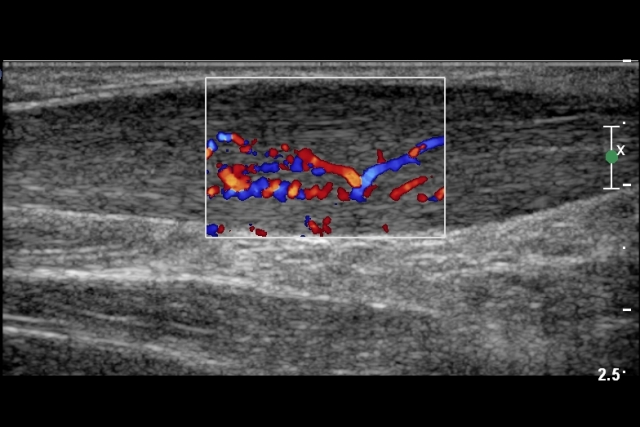

Shockwave therapy was first developed in the 1980s for breaking down kidney stones, but doctors soon noticed that the same sound waves also stimulated healing in bone and soft tissues. This led to its adoption in musculoskeletal medicine, where it is now widely used for chronic tendon problems and certain muscle and fascia conditions.
During treatment, a handheld device is placed on the skin over the affected area and delivers acoustic shockwaves into the tissue. These waves help increase local blood flow, stimulate cellular repair, and encourage the release of natural growth factors involved in tissue healing. In some cases, shockwaves can also help break down small calcium deposits that may be contributing to pain, particularly in shoulder tendons.
Tendon problems often persist because the tissue has reduced healing capacity and altered structure rather than ongoing inflammation. Shockwave therapy is thought to help “re-start” the healing response in these tissues, which can lead to reduced pain and improved function over time. Most patients receive a short course of treatments, usually spaced about a week apart.
Importantly, shockwave therapy works best when combined with an appropriate rehabilitation programme. While shockwaves may help stimulate biological healing and reduce pain, exercises are essential to restore tendon strength, improve movement patterns, and reduce the risk of symptoms returning. Your physiotherapist will guide you through a personalised loading and strengthening programme alongside your shockwave sessions.
Because it is non-invasive, shockwave therapy has minimal side effects and does not require injections or surgery. It can be a useful option for people who have not fully responded to standard physiotherapy and are looking to return more comfortably to work, sport, or daily activities.
Knee Bracing
Össur are an Icelandic company specialising in the development of innovative orthopaedic equipment including braces, supports and prosthetics.
I have received training in the fitting of several of their flagship braces, most notably the Unloader One, Unloader One X, and CTi OTS braces.
The Unloader braces have been proven to provide pain relief from osteoarthritis of the knee, and are recommended by many orthopaedic surgeons as a way of delaying surgery for as long as possible. Used on the right patient at the right time, they can be an incredibly effective component of management of an osteoarthritic knee, or degenerative meniscus tears.
The CTi OTS is most commonly used after ACL injuries, whether conservatively or surgically managed, especially for those who want to get back on the ski slopes. Again, it is a popular choice of brace for many of the orthopaedic surgeons who specialise in knee ligament reconstruction.
Fitting of these braces requires the taking of simple measurements, before the brace is then ordered in and fitted. If your consultant has recommended one of these braces, or if you have heard about them and wish to find out more, please contact me to discuss.
Ossur Unloader One®/Unloader One® X

Osteoarthritis- Ossur’s Unloader One, and Unloader One X have been designed specifically for patients who have pain from osteoarthritis on one side of the knee (known as unicompartmental osteoarthritis). Both the Unloader One, and Unloader One X improve mobility by providing pain relief from knee osteoarthritis and degenerative meniscal tears. They feature Össur's unique patented and clinically proven 3-point Leverage System that generates unicompartimental unloading of the knee joint
Ossur CTi

Ligament instability, or post ligament reconstruction- Introduced thirty years ago to stabilise and protect ligaments and cartilage, the tried and tested CTi design has evolved over time. The central concept, however, remains the same – a static support system consisting of a rigid frame and non-elastic straps. The CTi® OTS substitutes elements of the rigid CTi® frame with flexible subshells, providing adjustability and an excellent out-of-the-box fit while maintaining the level of support and protection that you would expect from a CTi® knee brace.